The post The sound of silence appeared first on Meaningful Care Matters.
]]>I grew up not being very comfortable with silence as that usually meant I was alone when I didn’t want to be, or worse, in trouble for doing something wrong. We were never yelled at as kids if we got into trouble. Instead, we were given ‘the silent treatment’ along with some time out in our rooms to think about what we had done. I remember wishing at times that my Dad would just yell at me and be done with it but in hindsight, the silence was probably more effective. As much as I had learned the awkwardness and discomfort of silence in those early years from my Dad, he also taught me in later life how important silence can be and that it is an integral part of communicating.
Fast forward forty years and I spent many days by my Dad’s bedside when he was dying. The visits weren’t easy, as I always felt that I needed to find things to talk about and do. I felt I needed to distract him by keeping busy, and I thought that was the best way to make my presence known and felt by him. I think I was also at some level trying to avoid and suppress my own sadness about what was happening. Dad would respond to some of those things and enjoy them briefly, but he also found it very tiring.
Sometimes, when I thought Dad was sleeping, I learned to sit quietly beside him without the pressure of words. By providing that silence, I suddenly started to notice that Dad would talk more and sometimes he would say very profound things about his thoughts and feelings about his life. This gave me a new window into learning things I didn’t know about him before, which I will always cherish. By being quieter myself, I literally gave him more space to initiate contact and say the things he needed to say before he died. It was a comfort to him to feel me beside him, sometimes holding hands, with no need to talk. The connection felt much deeper and more real. My brother would also visit, and he was similarly quite loud and busy. He would sometimes ask why our father seemed to talk to me more, so I encouraged him to slow down, listen and watch more, without filling the space with television, music and random chat. He struggled with this, as so many do. Learning the language of silence isn’t easy and takes time.
I would have missed out on so much if I hadn’t preserved or honoured the silence.

Consultant Trainer, MCM
The post The sound of silence appeared first on Meaningful Care Matters.
]]>The post The end of life appeared first on Meaningful Care Matters.
]]>Some people deal with this stage of their life in the same approach that they have gone through other stages of their life, and they like to do it “their own way”.
This leads me on to tell you about a gentleman I know who lives in a rural community who is nearing the end of his life and his personality for as long as I have known has been one of a gentle person who is what some would describe as a ‘loner’ and reclusive. His situation is one where he is refusing support as he is in fear of going to hospital or into a care home but will visit his GP at times. This gentleman has a special reason to keep going for as long as possible and for wanting to stay in his own home, as he is the main carer for his adult son who has learning disabilities since his wife died years earlier. Family and Health professionals want to help and care for him but his love for his son and his need to be there for him is so strong, together with his fierce independence, leads him to choose this path and this gives him hope and purpose to live out his life his way.
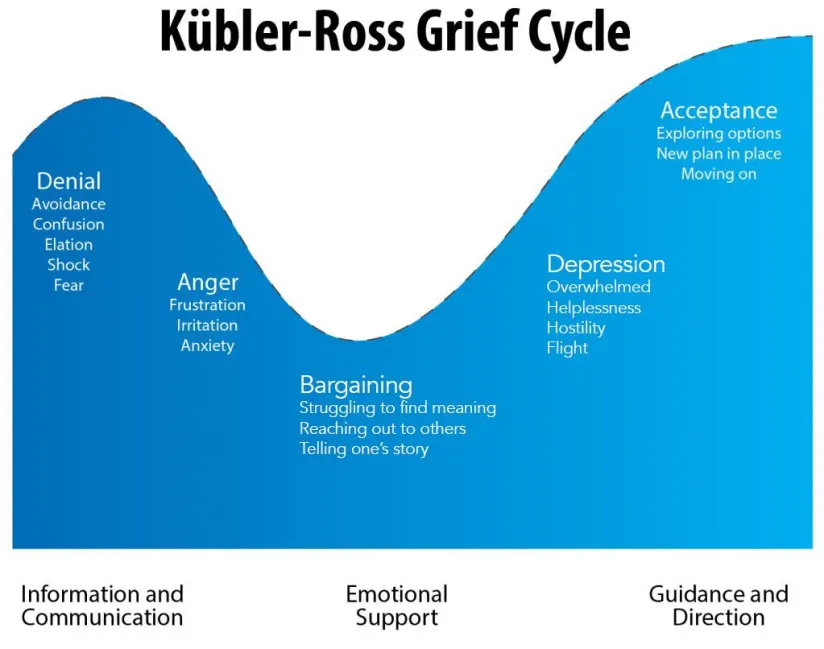
How do people process this stage in their life? For many it is very difficult especially if they are not ready and it is a process they go through as Elizabeth Kubler Ross (1969) who was a Swiss psychiatrist describes as the grief process which includes: Denial, Anger, Bargaining, Depression, and acceptance, but it should be noted that not everyone is able to work through all these stages.
For Health Professionals it can challenge our emotions and how we deal with difficult conversations whilst trying to support a person with a positive approach, at the same time feeling inadequate as we cannot “fix” it or make it right. What we need to remember is that this is their journey, and we are on it with them and a respect for their wishes and needs is paramount to their care. There may be questions on where to die? What happens when I die? what happens after I die? Who can I talk to about support for my family and my cultural beliefs. It is a gentle balancing act to ensure that information and support is provided but at the pace and depth that a person wants. Listening is key when trying to navigate the complex process of “the end of life.” We will not always get it completely right, but we do our best with love and respect.
These are some of the wishes made to me throughout my nursing career caring for people in their home, hospice, community settings and acute care.
George loved to have his little dog snuggle up on the bed with him, Audrey loved to listen to classical music with her husband, John enjoyed having his friends around his bed having a drink together and Heather loved to have a massage in her bed and then drift off into a relaxed peaceful sleep.
“You matter because you are you, and you matter to the end of your life. We will do all we can not only to help you die peacefully, but also to live until you die.”
Cicely Saunders

Nurse Consultant
MCM Canada
The post The end of life appeared first on Meaningful Care Matters.
]]>The post A compassionate approach to enhancing the quality of life appeared first on Meaningful Care Matters.
]]>On its surface, palliative care is when we treat the symptoms rather than the cause of the condition. We’ve accepted that the outcome is a one-way trajectory, and we look to make that journey as comfortable and meaningful as possible. I have worked in Long-Term Care as a nurse for several years, and I can tell you, that this journey begins, looks, and feels different for everyone.
While often associated with end-of-life care, palliative care is not limited to the final stages; it can be introduced at any point during an illness, including from the time of diagnosis. One of the core tenets of palliative care is symptom management. People grappling with serious illness frequently experience physical and emotional symptoms that can significantly impact their well-being. Health care providers should work collaboratively with the person, their family, and other healthcare professionals to alleviate pain and enhance overall comfort. This approach not only promotes physical relief but also contributes to an improved emotional state, creating a more supportive environment for both the person and their loved ones.
A holistic approach is another integral aspect of palliative care. Unlike traditional medical approaches that may focus solely on treating the disease, palliative care recognizes the multifaceted nature of well-being. It addresses not only physical symptoms but also attends to the emotional, social, and spiritual needs of individuals. By taking a holistic approach, palliative care strives to provide comprehensive support, acknowledging the interconnectedness of various aspects of life and health.
Effective communication is a cornerstone of palliative care. Open and honest conversations between the individual and their families are crucial for understanding preferences, goals, and values. These discussions enable the development of personalized care plans that align with an individual’s wishes. Clear communication fosters a sense of trust and empowerment, which in turn, enables the person to actively participate in decisions about their care.
Family involvement is a key component of palliative care. Serious illnesses affect not only the individual but also their loved ones. By involving family members in the care process, palliative care aims to create a supportive network that extends beyond the clinical setting, ensuring that the person’s needs are addressed in a comprehensive manner.
As I think about what lies ahead for my relative, and anyone that has been given the unimaginable prognosis of death, I find myself immersed in thoughts of how significant and personal this journey would be to any one person. By focusing on symptom management, adopting a holistic perspective, fostering open communication, and involving families, we can only strive to enhance the quality of life for them and their loved ones. Palliative care is a crucial component of healthcare that we hope empowers individuals to navigate their unique journey with dignity and compassion.

Associate Nurse Consultant, MCM
The post A compassionate approach to enhancing the quality of life appeared first on Meaningful Care Matters.
]]>The post Being You Until Your Last Breath: The Story of Pop appeared first on Meaningful Care Matters.
]]>I remember a sweet man from India that everyone referred to as Pop. He had been given that name by staff many years earlier as recognition of his caring and gentle nature, particularly when interacting with staff. His decline happened slowly over many years, but one day his death was before us. No matter how much you understand about dementia and the progression of this disease, you are never prepared when it’s time for people to leave, particularly those who held a special place in your heart, as Pop had with so many of the staff.
When Pop’s family were informed that his death was imminent, they said they would not be coming in as they felt the father they had loved and known left many years earlier; they were not unkind, just matter of fact. Staff immediately sprang into action. Their biggest fear was that Pop would die alone and without the things he loved. They wanted him to have a peaceful and loving death. Fortunately, this home was a Butterfly Home and staff were well versed in personhood.
Staff developed a schedule so someone was with Pop every moment (with many not going on break so they could be with him), they created the Pop Palliative Care Experience that included his favourite music, food, and smells. Pop was Hindu but none of the staff were, so they researched palliative care practices for that culture. They filled his room with music, incense and readings that would have been practiced if he had died in his home country. They held his hand, reminded him of things he had done and shared laughs and true feelings with him. When the moment of his death arrived, he was peaceful. As devastating as it was to lose an old friend, staff smiled and cried at the same time; they were going to miss him terribly but they knew they had given their friend a good death and they were there for him in his final days. Many years later staff still speak of Pop fondly, he was their family.
Mary Connell
The post Being You Until Your Last Breath: The Story of Pop appeared first on Meaningful Care Matters.
]]>The post What I’ve learned about dignity in dying appeared first on Meaningful Care Matters.
]]>I’ve learned that when you are not given effective comfort care, you’re in pain and struggle to breathe.
I’ve learned that when there’s no thought to your environment, you lie on an uncomfortable bed under bright lights with nothing to look at for hours on end.
I’ve learned that it doesn’t matter if you’re sensitive to noise, all you can hear is the banging of trolleys, loud voices, and call bells.
I’ve learned that for some, honour and respect of your person is not as important as getting the job done and moving on to the next.
I’ve learned that unless you have loved ones nearby, there’s much more clinical touch and much less for caring and comfort.
I’ve learned that if you feel scared and alone, the next person to check on you won’t be in for another hour or so.
I’ve learned that when you feel you have something to say but can’t speak, there’s no time to help you and no pen and paper on hand.
I’ve learned what it looks and feels like when you are no longer a person with a life story, you’re just a bed number with a chart.
I’ve learned through my brother’s experience that there must be a better way! A way to die with dignity and hope while still feeling connected to those we love.

Consultant & Trainer
MCM
The post What I’ve learned about dignity in dying appeared first on Meaningful Care Matters.
]]>The post Dying with Love and Dignity appeared first on Meaningful Care Matters.
]]>How do we die? why me? why now? I am frightened of dying, I am angry, how will my family cope without me? I want to see my children get married, I wanted to have children, but it is too late now. I have had a good life, I am ready to join my husband, I am ready to go now I feel at peace. I am tired off the pain, I want to consider medical assistance with dying, as I want control over my death.
These are some of the comments made to me as a registered nurse throughout my many years caring for people who were dying in the community, hospice, and acute care.
When we are living, we want love and dignity so why should it be different when we are dying? It can appear complicated and overwhelming for the person, families, and friends in how to achieve this.
We have our own personal qualities and attributes which make up who we are. We have our own values and belief systems and for as long as we are able, we have the right to choose what is important to us as a person based on those beliefs and what we truly believe is ‘dying well’. When we are unable to control what this looks, sounds, smells and feels like we all have a role to play in facilitating a death that embraces love and dignity. Is there a right and wrong way to do this? And do we all see love and dignity in the same way?
Love and dignity come in many configurations such as privacy, laughter, family, friends, lovers, pets, respect, music, singing, quietness, touch, smells, makeup, special clothes prayer, spirituality, and acceptance.
For Jennifer it was having her family and friends ‘hang out’ with her and for her to take in and enjoy the ‘banter’ humour, story telling and ‘belly laughs’.
For George it was enjoying his honeymoon with the love of his life who he married whilst in the hospice and staff decorated the guest room into a honeymoon suite and pushed the two beds together.
For Joan it was the serenity of listening to classical music, having aromatherapy oils burning, family coming in and out and having hand massages from staff.
For Francene it was having her adult children singing together in harmony whilst sat around her bed.
As we leave this world, the gift of dying with love and dignity is the greatest gift than can be bestowed upon us.
“Unable are the loved to die, for love is immortality.”
Emily Dickinson

Consultant and Trainer
MCM Canada
The post Dying with Love and Dignity appeared first on Meaningful Care Matters.
]]>The post Dying a Good Death appeared first on Meaningful Care Matters.
]]>We use the words ‘dying’ or ‘terminal’ to describe when a person is in the last few days or hours of life. Sometimes a death is sudden and unexpected. For some family members of a loved one living with a dementia, saying goodbye occurred years ago. What is a good death? Is it filled with love?, Is it a right of passage?, Is it filled with rituals?, Is it freedom? Or is it a privilege?
As an ageing population, there is no escaping the fact that there will come a time when we will leave this world behind. Quality of care will be at the top of our personal agenda, whether it’s for a loved one or because we, ourselves, need support. The end won’t be a surprise for with living comes dying for us all.
Let’s talk about dying a good death.
Conversations About Death
Society still harbours a taboo when talking about death. As a nurse I do get to have conversations about death, and they are always powerful. Yes we discuss end of life we are talking but if you listen closely, what we really talk about is the gift of life, the value we place on it and the appreciation we have acquired for its fragility.
It’s time to get this conversation started.
By encouraging people to start talking about the end of life our goal, is to encourage us all to feel comfortable talking about death, more importantly planning for a good death. By this I mean what you envision, how you want to be treated, things you do want and things that you don’t when it is your time to die. These are important conversations, I know, I have seen what a bad death can look like with well meaning people inflict their needs and wants onto the dying person, without any consideration of what they might actually want or need.
Death brings out the best and worst of moments of our humanity. It’s raw, emotional, and exhausting. BUT… what if we took the time to sit down with the people we loved and asked them what their wishes are at the end of their life? Let’s break the taboo and discuss death. This is the first step in creating a good death.
How To Die Well
Physical pain vs Spiritual pain.
Being pain-free is more than physical, it’s spiritual. Medications can manage most people’s physical pain well however, spiritual pain is more complex. Easing spiritual pain can be accomplished by acknowledging the spirituality the person. Not one size fits all, understanding spirituality is not about religion or culture, but, it could be. Spiritual issues are common at the end of life, it’s better to have someone who can engage in meaningful spiritual questioning. A good death is one which can reconcile the feelings and emotions of one’s core spirit in a way which is not impacted by others spiritual bias.
Psychological pain.
We must also recognise psycho-social pain, the residue of life’s unresolved conflicts with other people, places or things. Interpersonal conflict is a reality for us all. It is important to acknowledge those conflicts and feelings that are unresolved and process them to the best of our ability. There are four basic ways to address psychological conflicts at the end of life:
- Love conquers all.
- Forgiveness is a way to heal the mind, soul and spirit.
- Acceptance is comforting.
- Reconcile regrets.
A good death creates a space for addressing the hidden mysteries of life.
Satisfy any remaining wishes.
Some people want to live long enough to see something come to pass. Look at the things you need to resolve and the things you need said or done before they become a burden that can’t be overcome. Find your inner peace and let go of any burdens you feel. This is what freedom feels like.
Every life has meaning, celebrate it.
There are two main ways that people on their deathbeds find meaning: in the recognition of all of the people they have loved and who have loved them, and in the work that they’ve done that has contributed to the greater good. Articulating what brought meaning to life will support all to die well.
Be protected from dehumanising procedures.
Know what you want and what you don’t. Dignity in death is having control over the experience. Be mindful many clinical supports work to preserve life. Be clear about what clinical practices you want and when. Be persistent and clear to avoid procedures that are unwanted. Be a positive vocal advocate and create an experience that is meaningful and right for the person.
Final Thoughts
Dying gives us the chance for the most glorious embrace of all. When that happens, it is a good death.
If I should go tomorrow
It would never be goodbye,
For I have left my heart with you,
So don’t you ever cry.
The love that’s deep within me,
Shall reach you from the stars,
You’ll feel it from the heavens,
And it will heal the scars.

RN (Australia)
Managing Director MCM
and Grandson of wonderful human beings who lived with dementia
REFERENCES
Meier EA, Gallegos JV, Thomas LP, Depp CA, Irwin SA, Jeste DV. Defining a Good Death (Successful Dying): Literature Review and a Call for Research and Public Dialogue. Am J Geriatr Psychiatry. 2016 Apr;24(4):261-71. doi: 10.1016/j.jagp.2016.01.135. Epub 2016 Jan 22. PMID: 26976293; PMCID: PMC4828197.
Lawrence, V., Samsi, K., Murray, J., Harari, D., & Banerjee, S. (2011). Dying well with dementia: qualitative examination of end-of-life care. The British Journal of Psychiatry, 199(5), 417-422.
Chu C. (2019). Normalising conversations about death and dying. BMJ. 366:1504. Doi:10.1136/bmj.15041.
The post Dying a Good Death appeared first on Meaningful Care Matters.
]]>The post What Dad taught me about acute care, dying and grief. appeared first on Meaningful Care Matters.
]]>3rd October 2022, my father had a heart attack. I was there to witness it. Less than two hours later, my Mum and I sat in Broad Green Hospital in Liverpool thinking this was it. He’d had chest pains, but we had to wait two hours for an ambulance. He told my Mum he loved her, as if preparing himself. Incredibly, he survived. He didn’t remember the attack itself. The NHS is incredibly hard pressed, but what those staff did for my Dad and our family was amazing. He received incredible person centred care as we all did when he passed away peacefully after a stroke in January this year. What do I mean by person centred care in this case? It was obvious that they were incredibly busy, but they always had time for Dad. They treated him with respect. As a fellow human being. Husband. Father. Grandfather. It came from the head and the heart. There was dignity.
Like most people, I dreaded the thought of losing a parent and what was unexpected was how I felt afterwards and how I feel now. Yes, I did buckle with grief on more than one occasion, but what I wasn’t expecting was a sense of relief and freedom. Should I feel guilty about that? No, I don’t think so. I love my Dad and it makes me sad to see what my Mum is going through. You just don’t know how someone will be or react to the death of someone close or even one’s own impending mortality. There was no way my Dad would talk to me about it. That was his choice. I respected that.
In a care setting everyone there will have very different reactions and means of dealing with death. Some may seem inappropriate or gauche to others. Too little. Too much. I am no advocate of the ‘stiff upper lip’, but the cult of showing emotion as a competitive sport leaves me cold. You should feel sad, you should happy’. Our feelings are our own and don’t belong to anyone else. I want to enable people to be authentic, to be real about how they feel. I’m working on that one.
That feeling of freedom I mentioned earlier, is I think about seeing Dad free from pain, that in the end it was a deserved peaceful end for a life where he gave much more than he received. To be honest, I can’t find a word to express how I feel. it changes.
I heard someone on the radio today, express their feelings about death. It’s what I’m trying to aim for and is strangely similar to the words I used in the eulogy at this funeral.
‘Don’t be sad for what you have lost. Be happy for what you have had.’

Consultant Learning & Development Manager
MCM
The post What Dad taught me about acute care, dying and grief. appeared first on Meaningful Care Matters.
]]>The post Natalia’s Story appeared first on Meaningful Care Matters.
]]>Natalia is a Registered Nurse (RN) and Team Leader for the Butterfly houses at Sunnyside Home, Region of Waterloo. Natalia, a native of Colombia, was interested in pursuing a career where she could help people. Natalia didn’t start off wanting to be a nurse, she started her journey in medical school before an experience changed her life.
During a student placement, Natalia cared for a patient who was dying of AIDS. “I watched him die a horrible death” explained Natalia. “I tried to tell them that he was in distress and no one listened.” Natalia felt that she didn’t have a voice. “Nobody cared, I hated nurses back then”. Natalia had to make a choice, run from the “business of healthcare”, or face it head on and work towards a better future. “I knew I could do better,” so Natalia left Colombia and travelled to Canada to pursue nursing.
Caring for older adults with dementia was natural for Natalia. Reflecting on her early days working as an RN at Sunnyside Home Natalia explains, “Whenever I was stressed out, I would go to the [dementia care] areas to get hugs and spend time with people.” When the opportunity presented itself to become the team leader for these areas, it felt like a perfect fit.
Natalia co-chairs the Palliative Care Committee at Sunnyside alongside the Chaplain. This interdisciplinary team has built a program that focuses on A Palliative Approach to Care. This approach focuses on comfort and quality of life by supporting an individual holistically and not just their clinical needs. It involves open and honest communication with families about what to expect when caring for someone with a chronic condition. People are supported as individuals to live their best life in the time they have left and to die a good death when the time comes.
Planning and communication is important in dementia care because it gives families time they need to prepare and to find moments of connection with the person they support. This doesn’t change what we do at the end of the life to keep people comfortable but it helps support a meaningful life along the way.
Natalia notes that A Palliative Approach to Care aligns with The Butterfly Approach by encouraging people to be more flexible. “It opens doors and helps people let go of control,” says Natalia. “They want a beer? Give them one! Ice cream? Why not? They want a hotdog? We’ll puree it or mince it [if that’s what they need].” By doing this “we feel like we’ve accomplished something, supported them until the end.”
Looking back, what advice would Natalia offer her younger self? “It’s never wrong to advocate… I was too shy back then, not wanting to stir the pot. Now I’m a little more assertive.” Natalia’s advocacy has an impact. “Families have been very thankful for the preparation and support that they receive and that we give them enough time to be there for those moments. It does make a difference.”
The post Natalia’s Story appeared first on Meaningful Care Matters.
]]>The post Empty Seat at the Table appeared first on Meaningful Care Matters.
]]>I have a Christmas Eve tradition of sharing a Facebook post, reflecting on the year (including my work as a dementia care trainer/consultant) and remembering those who will be absent from the table during the festive season, following bereavement.
I see this through the prism of celebrating lives lost. However, as I age, the list of names seems to grow – particularly those whose dementia journey has ended.
We are all different, so loss can feel like an intensely unique experience.
The Loss Spectrum
Carers of people with dementia (relatives/friends/significant others) experience a kaleidoscope of losses:
- initial diagnosis
- progression of their loved one’s illness, sometimes perceived as that person ‘disappearing’ or ‘no longer the Mum I remember’
- transition into residential care – one daughter told me “This was the worst day of my life”
- ‘she/he no longer recognises me as their partner/spouse/child etc.’ – perhaps, the most painful of experiences
- their loved one’s death
Indeed, over many years of working with carers of people with dementia, I’ve heard the expressions – “it’s like the longest bereavement” or “it’s a constant grieving process” – countless times.
Examples of loss can feel profoundly personal and unique for individual carers.
Patience’s journey began with supporting her husband through his acute anxiety during his forties, a later diagnosis of Parkinson’s Disease, then Parkinson’s-related Dementia and his recent death. Her story is a long one with many different losses and stresses along the way.
In the Rainbow Memory Café for older LGBT+ people who have dementia and their carers, Christopher, recently shared how he is still coming to terms with the death of his husband with whom he had lived for 40-plus years. Unlike many others, he’d felt supported by family and friends, yet the sense of loss remains overwhelming: “immediately after Joe died, all the professionals went.” It is not uncommon for relatives to describe this sudden shift of a busy home with lots of visitors to so much more silence and hours of time in the day to fill.
Meanwhile, Kate has been experiencing the anguish of her mother Jenny moving into residential care, trying to ensure she has prunes for breakfast, as she knows Jenny best and that this is important to her.
Many families have to navigate developing positive relationship with care staff and want to make sure their relative has what they need, but are worried about being labelled as difficult or interfering.
Unique or Universal?
It is often those ‘simple things’ – laying a second place at the table and then realising that our loved one is no longer there or feeling vulnerable and in need of a loved one’s holding hand or hug.
Such moments of personal grief and emotional pain, I’d suggest, are actually universal feelings when dealing with loss, including bereavement.
Loss and bereavement remain taboo topics for discussion, despite being a certainty of life. Their mention simply reminds of our own mortality and difficult feelings. The emotional pain of bereavement is not something we ‘get over.’ Rather, it is a reality of life that we can only hope to adjust and adapt to.
Nevertheless, as light follows darkness and spring follows winter, we can still remember and celebrate lives. My mother and father-in-law both died in 2020. For Christmas 2022, on behalf of the family, I donated to have 5 trees planted in their memory. Hopefully, a symbol that whilst they are no longer ‘at our table’ our love for them remains.

Associate Trainer
MCM
The post Empty Seat at the Table appeared first on Meaningful Care Matters.
]]>